



- Clinical context often breaks down as data moves between documentation, coding, billing, analytics, and AI systems
- Missing connections between encounters can lead to inconsistent coding, reimbursement challenges, operational inefficiencies, and weaker downstream data quality
- These issues stem from how healthcare technologies capture and structure clinical information across workflows
- Knowledge graphs help maintain continuity by linking symptoms, diagnoses, treatments, and outcomes within a connected clinical framework
Health technology companies have an opportunity to improve customer outcomes by reducing the loss of meaning that occurs as information moves across systems.
Platforms that preserve clinical context can support cleaner claims, more consistent data, improved operational efficiency, and more reliable AI and analytics performance.
IMO Health’s Knowledge Graph enables this by connecting clinically validated concepts across documentation, coding, billing, and analytics workflows – helping preserve meaning and improve continuity throughout the care journey.
Healthcare data travels through a complex network of systems. Documentation, coding, billing, analytics, and research each rely on it. But along the path, clinical intent isn’t always preserved. Differences in terminology, missing context, and disconnected records create inconsistencies that flow into downstream functions.
The impact shows up quickly. Documentation becomes harder to align across encounters. Coding varies. Claims require rework. Data becomes less reliable for analytics, artificial intelligence (AI), and research.
One of the most promising ways to address this challenge is to invest in a connected foundation for clinical data – in other words, a healthcare knowledge graph. This type of solution links symptoms, diagnoses, treatments, and encounters into a shared context, ensuring information remains consistent at each step.
The difference becomes clearer when you look at a single patient journey, as illustrated in the example below.

When a sore throat leads to surgery
An 8-year-old patient, Alex, presents with a sore throat. Then it happens again. And again.
Over the course of 14 months, those recurring symptoms lead to four separate encounters and eventually, a surgical evaluation.
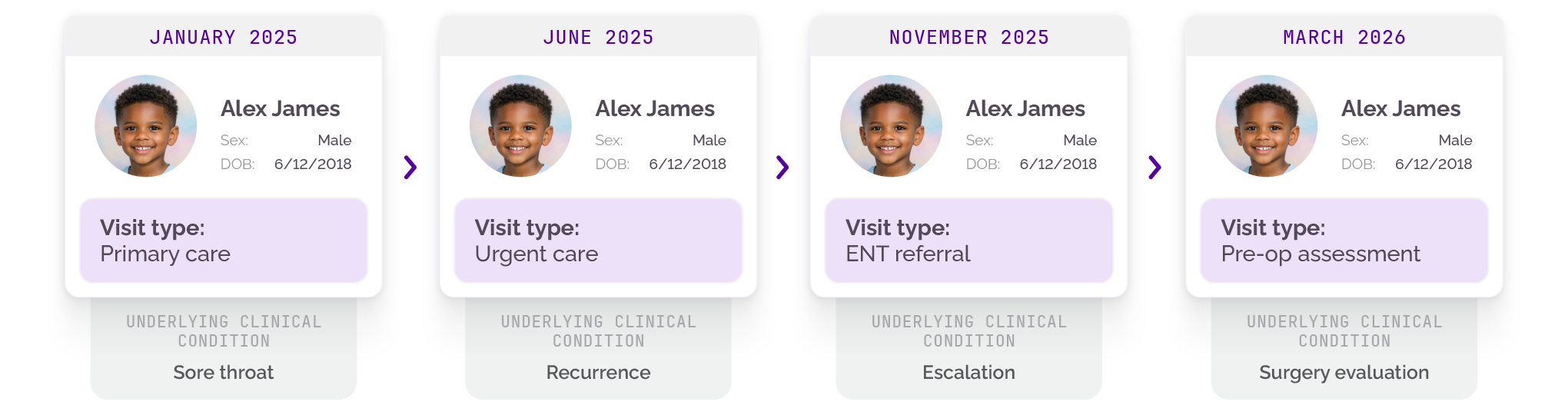
On the surface, it’s a familiar clinical story. Underneath, it’s a fragmented journey where meaning doesn’t always carry forward; the same journey can unfold differently depending on how the data behind it is structured.
In one scenario, each visit stands alone. In another, each encounter builds on the last.
|
|
|
|
|
|
|---|---|---|---|---|
| Without a knowledge graph | History re-collected | Generic or unspecified | Higher denial risk | Delays and rework |
| With a knowledge graph | History connected across visits | More specific, accurate coding | Cleaner claims | Faster, more confident decisions |
The journey behind each visit
Each encounter in Alex’s journey is only one part of the story. Behind it sits a chain of steps: documentation, diagnosis, coding, billing, and coordination.
At every stage, information is captured, interpreted, and passed along. When that information is incomplete or inconsistent, it affects future visits.
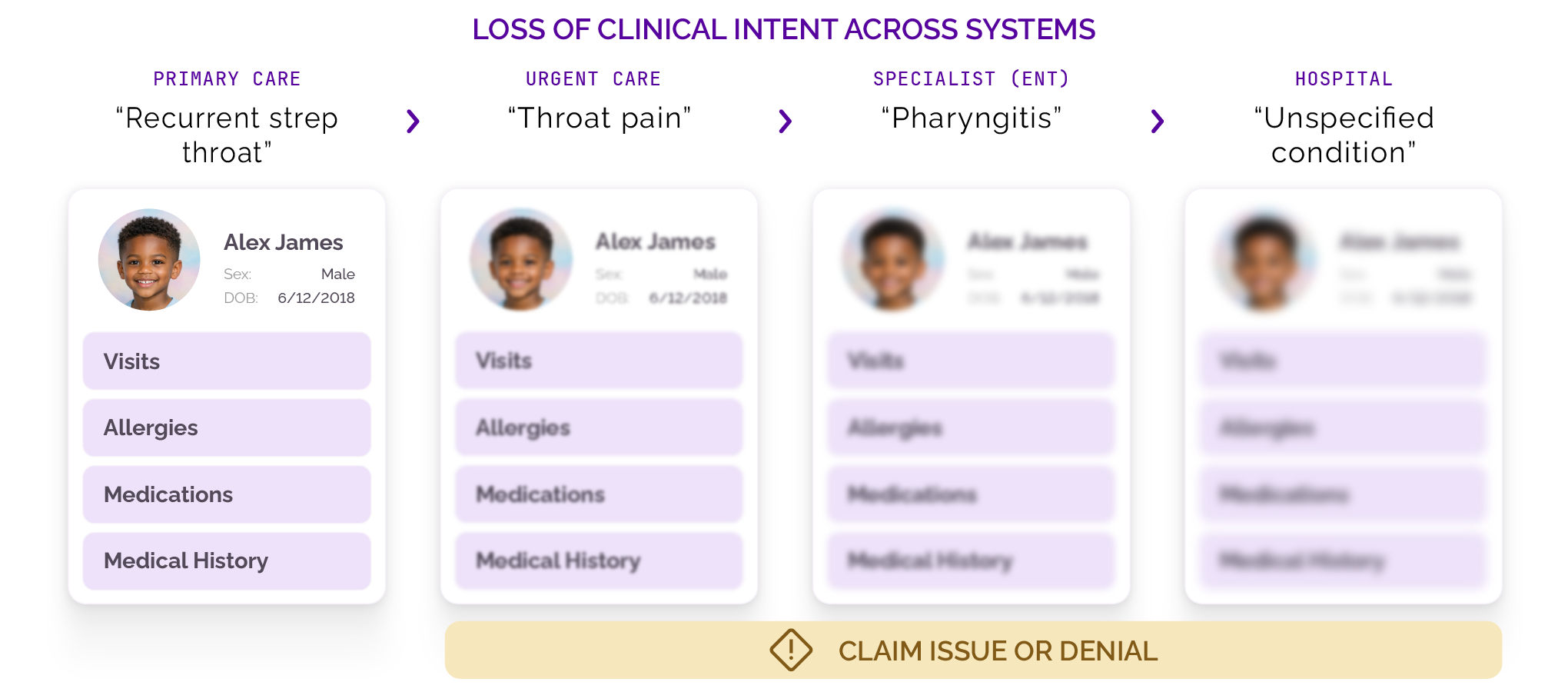
Where meaning starts to slip without a knowledge graph
As Alex’s medical information moves through then healthcare system, clinical intent shifts. What begins as a clear and specific picture at the point of care becomes less precise as it’s translated into structured data, codes, and downstream workflows.
Differences in terminology, missing context, and disconnected records all contribute to this drift, making it harder to track Alex’s condition reliably.
For example, at one visit, his provider notes “swollen glands” and “lymphadenopathy of head AND/OR neck,” but these get flagged as “not a finding” in the electronic health record (EHR) when the context isn’t recognized – either because it isn’t explicitly captured or because there is no system in place to interpret it consistently.
A few encounters later, “oropharynx hyperemic with purulent exudate” gets coded inconsistently across EHRs (one system codes J03.00 for acute streptococcal tonsillitis, unspecified; another defaults to J03.9 for acute tonsillitis, unspecified).

What this means for health tech teams
- Inconsistent inputs lead to inconsistent product behavior across applications
- Data models struggle to reconcile differences in terminology and context
- AI and analytics systems inherit gaps, reducing reliability and explainability
The ripple effect of lost meaning
When clinical intent isn’t preserved, the consequences are immediate and costly – and they show up differently across teams.

Clinicians may document a clear pattern, such as recurrence over time with justified escalation. Coders may struggle to interpret that pattern from incomplete or inconsistent inputs. Billing teams may lack the specificity needed to support medical necessity for prior authorization.
As a result, teams spend time reworking documentation, clarifying diagnoses, and resubmitting claims. Denials increase due to missing specificity or incomplete histories. In one study, 1.5% of pediatric tonsillectomy claims were denied post-prior-auth1, with an overall denial rate of up to 15% among private payers.2

What this means for life sciences organizations
- Fragmented data limits accurate cohort identification
- Loss of context reduces the quality of real-world evidence
- Inconsistent terminology makes it harder to link clinical and molecular insights
For Alex’s family, this means delayed surgery, repeated ER visits, school absences, and parental frustration. For health systems, this translates to operational inefficiency ($25–$118 per denied claim in rework), revenue leakage (up to 12% of hospital revenue at risk), and added administrative burden.3
Patient safety suffers too – 18% of EHR-related incidents trace to interoperability failures that strip context from clinical documentation.4
How does a knowledge graph change the patient journey?
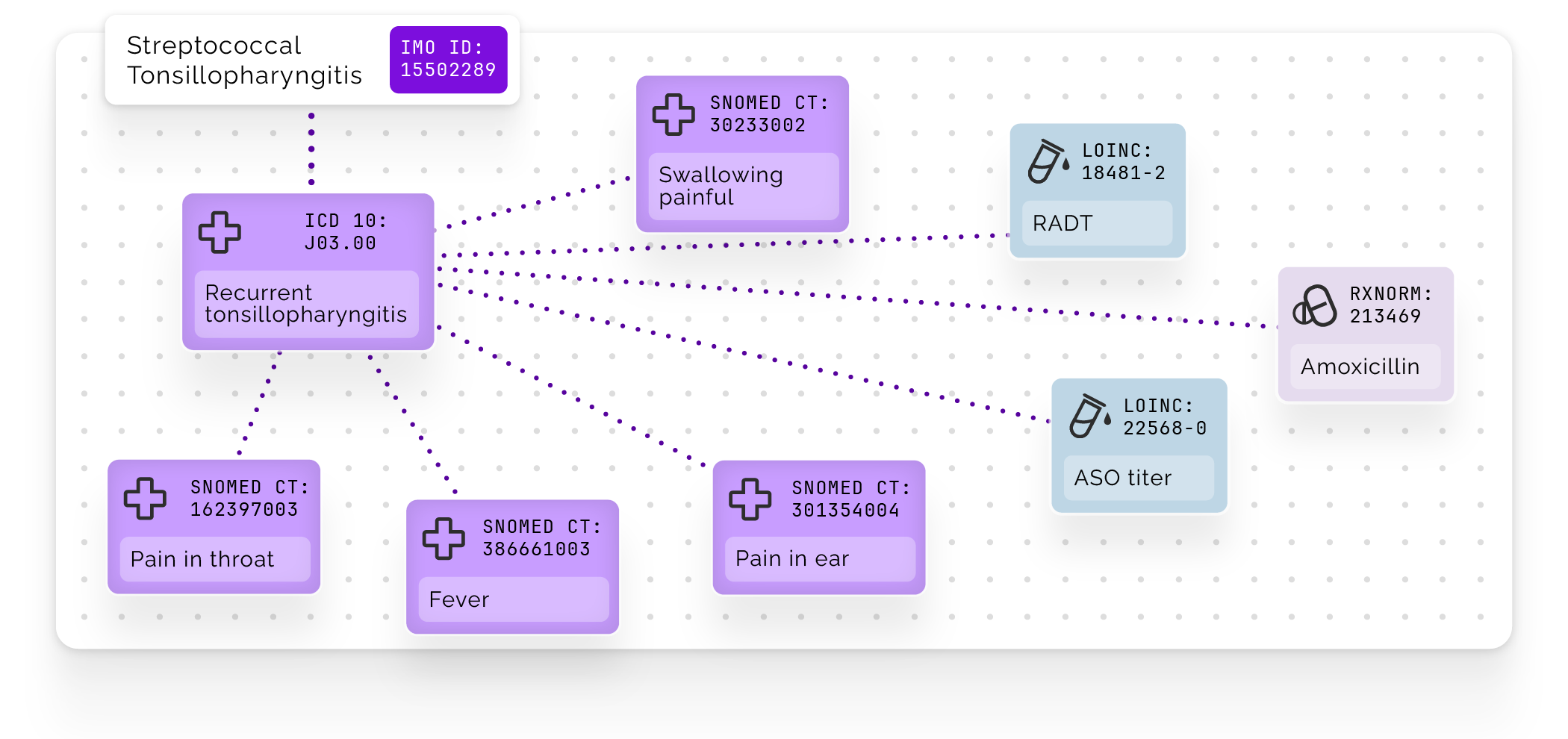
A clinical knowledge graph connects clinical concepts – such as symptoms, diagnoses, treatments, and outcomes – into a structured, contextualized network. Instead of treating each data point as isolated, it preserves the relationships between them.
But not all knowledge graphs are created equal. Without deep clinical grounding, even well-structured data can lose meaning over time.
To be effective, a knowledge graph must be built on a foundation of clinically validated terminology, mapped across standards (such as SNOMED CT®, ICD-10-CM, and others), and enriched with both explicit and inferred relationships.
This kind of structure allows the graph to reason, not just connect data. It can preserve clinical intent, reconcile differences in terminology, and maintain consistency as information moves across documentation, coding, billing, and analytics.
It also serves as a critical grounding layer for AI, enabling systems to validate outputs against a structured representation of clinical knowledge – improving accuracy, explainability, and trust.
For a more technical overview, check out the following blogs:

Why this matters beyond the point of care
- Health tech: Enables scalable data models, cleaner integrations, and more predictable product behavior
- Life sciences: Supports richer datasets for research, cohort analysis, and precision medicine
- Across the continuum: Creates a consistent, explainable foundation for decision-making
A connected journey, end to end
Let’s take a key moment in Alex’s journey: a third visit with recurring symptoms. At this point, his symptoms reflect a pattern rather than an isolated event.
With a knowledge graph, that same moment looks different. The clinician doesn’t need to reconstruct Alex’s history at the point of care, the coder has the specific information needed to assign a diagnosis, and the billing team has the documentation to support it.
That impact doesn’t stop at a single encounter. Across the full patient journey, the difference is cumulative.
Without a connected foundation, information resets at every encounter, requiring re-interpretation. With a knowledge graph, Alex’s fragmented 14-month journey becomes a continuous, trustworthy record that builds on itself over time.
A knowledge graph helps ensure clinical intent remains intact across encounters. It reduces rework, supports more accurate coding and billing, and improves the reliability of downstream data.
To learn more about how IMO Health’s proprietary Knowledge Graph transforms fragmented data into connected, clinically meaningful insight, click here.
SNOMED and SNOMED CT are registered trademarks of SNOMED International.
1Torrecillas, Vanessa F et al. What Is the Impact of Prior Authorization on the Incidence of Pediatric Tonsillectomy?. Otolaryngol Head Neck Surg. 2021;164(6):1193-1199. doi:10.1177/0194599820969631. Accessed via: https://pubmed.ncbi.nlm.nih.gov/33170763/
2Lagassi, Jeff. Revenue cycle challenged by low collection rates, high denials. Healthcare Finance News. Feb 28, 2025. Accessed via: https://www.healthcarefinancenews.com/news/revenue-cycle-challenged-low-collection-rates-high-denials
3Force-Ludwig, Jami. The High Cost of Denials: How Prior Authorization Challenges Are Draining Your Bottom Line. NYX Health. May 28, 2025. Accessed via: https://nyxhealth.com/the-high-cost-of-denials-how-prior-authorization-challenges-are-draining-your-bottom-line/
4Li, Edmond et al. The Impact of Electronic Health Record Interoperability on Safety and Quality of Care in High-Income Countries: Systematic Review. Journal of medical Internet research vol. 24,9 e38144. 15 Sep. 2022, doi:10.2196/38144. Accessed via: https://pmc.ncbi.nlm.nih.gov/articles/PMC9523524/


